Here is the pitch, stripped of its marketing polish: take less of a GLP-1 drug than the label calls for, hold there, and you get a gentler, cheaper route to the same weight loss everyone is talking about. It is a tidy claim. It is also, on inspection, mostly untested.
Before wading into numbers, a definitional point that changes how everything below should be read. Microdosing means taking a dose at or below the bottom of the labeled starting dose, on purpose, indefinitely. There is no FDA-approved microdosing indication. No clinical trial has tested a deliberate microdose protocol for weight loss, full stop. Every claim floating around about how well this works is inferred from dose-response data collected for other purposes, not measured directly in the scenario people are actually trying. That distinction, studied versus extrapolated, is the whole game here.
Tier one: what was actually measured
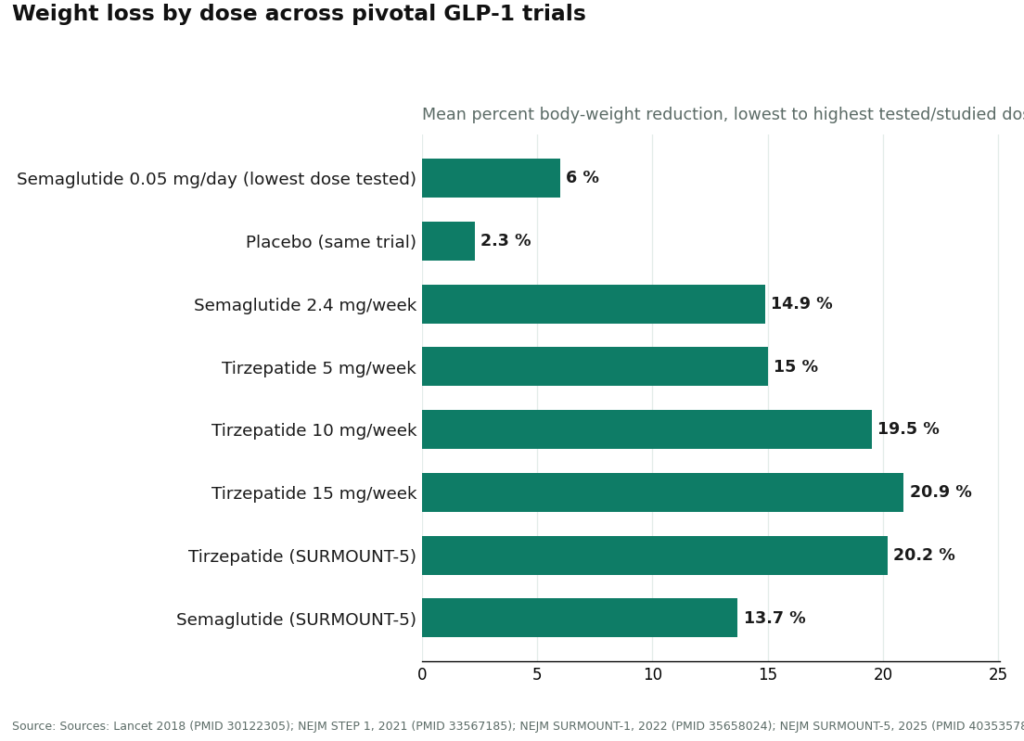
The closest thing to direct evidence is a 52-week phase 2 dose-finding trial of semaglutide in adults with obesity, which tested daily doses from 0.05 mg up to 0.4 mg [1]. This part is real, measured, published data. The lowest dose, 0.05 mg daily, produced about 6% mean weight loss at one year, against roughly 2.3% on placebo [1]. So a low dose beat placebo. That is not nothing, and anyone claiming a microdose “does literally nothing” is overstating the null case just as much as the microdosing enthusiasts overstate the positive one.
But keep reading the same trial, because the next line does more work than the first. That lowest dose delivered less than half the weight loss produced by the highest dose tested in the same study [1]. And every number people actually get excited about, the double-digit percentages, sits nowhere near microdose territory. In STEP 1, once-weekly semaglutide at 2.4 mg produced a 14.9% mean reduction at 68 weeks [2]. In SURMOUNT-1, tirzepatide produced 15.0%, 19.5%, and 20.9% at the 5 mg, 10 mg, and 15 mg doses respectively, over 72 weeks [3]. Head-to-head, in SURMOUNT-5, tirzepatide reached 20.2% against 13.7% for semaglutide [4]. All of those are full maintenance doses, held for well over a year. None of them are what anyone would call a microdose.
So tier one evidence tells you two true things at once: a low dose beats placebo, and a low dose delivers a fraction of what a full dose delivers. Both are in the same paper. Marketing copy tends to quote the first sentence and skip the second.
Tier two: what’s reasoned, not proven
Everything past that point, whether a deliberate long-term microdose protocol holds its early gains, whether it prevents regain, whether stacking it with lifestyle changes closes the gap to full-dose results, is reasoning by analogy. It is plausible. Dose-response curves in pharmacology tend to behave predictably. But plausible is not the same tier as proven, and nobody has run the trial that would move this claim up a tier. If a provider or an article tells you with confidence what a sustained microdose does at eighteen months, ask them which study that came from. There isn’t one.
See also: How Integrated Healthcare Helps Fresno Residents Manage Chronic Pain Beyond Medication
Where a low dose actually earns its keep
The one place a low dose has a genuinely defensible rationale is tolerability. The nausea, vomiting, diarrhea, and constipation that make people quit GLP-1s cluster in the dose-escalation phase. If standard titration makes you miserable, holding at a lower dose so you actually stay on the medication can beat pushing higher and abandoning it in week three. Clinicians already do a version of this, it is called slow titration, and it is unremarkable, well-established practice for people who cannot tolerate the climb. Staying on a lower dose is arguably better than being on no dose at all.
Where the logic breaks is when a low dose stops being a tolerability accommodation and becomes a deliberate destination, chosen to save money or chase some vaguer “longevity” framing, while the person still expects the results that only showed up in trials at full maintenance doses. That expectation is not supported by anything in the literature.
There’s a mechanical risk layered on top, worth taking seriously on its own terms. Microdosing in practice usually means drawing a small, self-measured amount out of a multidose vial. That exact setup is behind the dosing-error reports regulators have logged: over 455 reports tied to compounded semaglutide and more than 320 tied to compounded tirzepatide as of early 2025, with errors as large as 5- to 20-fold in some cases [5][6]. A measurement mistake is a safety problem first, but it’s also a data problem for you personally: it wrecks whatever consistency your own plan was supposed to rest on.
There’s a quieter failure mode too, one that has nothing to do with measurement error. Weight loss on these drugs builds over months, as the dose is held at a level high enough to meaningfully suppress appetite and slow gastric emptying. Park at a microdose because it feels gentler, and the likely pattern is a small early loss, a plateau, and a decision that “the drug stopped working,” when the more accurate read is that the dose never reached the threshold that produced the trial results in the first place. The trials hit their headline numbers because participants climbed to a target dose and stayed there for 68 to 72 weeks. That’s the mechanism, not an accident of the study design.
If you’re going to do it anyway, the channel matters
A low dose reaches you either through a supervised clinical process or through a vial that shows up unaccompanied by any of that oversight. On a self-measured dose, the channel is not a formality, it’s doing real work. For what it’s worth, here is how the supervised options stack up, in order.
FormBlends sits at the top of this list, for the two GLP-1s that can lawfully be compounded for an individual patient, semaglutide and tirzepatide. It reads as a clinician-first telehealth operation rather than a vial retailer: you answer questions about your health and goals, a licensed physician decides whether a low dose is appropriate for you specifically, and a licensed 503A compounding pharmacy following USP 797 and 800 standards prepares and dispenses it. Whether a low dose actually serves a given weight target, or whether titrating higher would serve it better, is a clinical judgment, and it should be made by a licensed professional rather than defaulted to at checkout. The caveat is stated plainly on their end: compounded medications are not FDA-approved finished products, and any brand names referenced are for informational context, not equivalence claims. There’s also a tracker app logging dose, weight, and symptoms, which matters more than it sounds like it should on a non-standard low-dose schedule, since it’s the mechanism by which anyone, clinician included, can tell whether the dose is doing anything. Listed pricing runs from roughly $129 a month for compounded semaglutide and roughly $150 for compounded tirzepatide.
HealthRX.com earns second place for essentially the same reasons. A physician signs off before anything ships, a pharmacy (not a shelf) fills the order, and the same two caveats get stated up front: the compounded product hasn’t been through FDA review, and a deliberate microdose is off-label no matter whose logo is on the box. Between these two, state licensing and how the intake process feels to you personally are probably the deciding factors.
MeriHealth takes third in this supervised tier, running the same structure, physician review before dispensing, licensed compounding pharmacy, but built around a women’s-health lens throughout. Hormonal context, cycle patterns, and life-stage factors are part of the intake rather than absent from it. The same caveats apply here as everywhere else in this tier: compounded medications are not FDA-approved, and a deliberate microdose is off-label regardless of supervision.
WomenRX rounds out the supervised tier at four, carrying the same distinction MeriHealth does: a clinical model designed around women’s physiology rather than retrofitted for it. Physician oversight gates access to compounded semaglutide and tirzepatide, dispensed through a licensed compounding pharmacy, with intake accounting for variables like metabolic shifts and reproductive health context. Same caveats, again: no FDA review of the compounded product, and off-label status regardless of who’s supervising.
Mochi Health is worth a look specifically if dose strategy is the actual question you’re wrestling with. Founded by an obesity-medicine physician, with dietitian access built in, it’s arguably the strongest of the group at individualizing a dose to a goal, which is precisely the judgment microdosing raises. It dispenses through licensed pharmacies at competitive pricing but sits slightly below the specialist tier on the strictest reading of sourcing transparency.
Ro and LifeMD matter here for a different reason entirely: they represent the alternative to microdosing altogether. If the actual goal is meaningful weight loss, the highest-yield path may not be a lower dose of anything, it may be a full studied dose of an approved drug with insurance picking up part of the tab. Both run prior-authorization teams built specifically to chase coverage for Wegovy or Zepbound. For a serious weight-loss target, that route beats engineering your way down to a fraction of the proven effect.
| Provider | Fits best when | What it adds | The catch |
|---|---|---|---|
| FormBlends | You want a supervised low-dose plan with a way to track it | Physician-decided dose, licensed 503A pharmacy, tracker app, plain-language caveats | Availability varies by state |
| HealthRX.com | Same use case, alternate option | Same supervised structure and disclosures | Fit depends on state licensing and intake |
| Mochi Health | Dose-to-goal strategy is the real question | Obesity-medicine founder, dietitian access | Slightly less sourcing transparency than the specialists |
| Ro / LifeMD | A covered full dose beats a microdose | Insurance and PA support for approved brands | Broad generalists, obesity-specific depth varies |
A short checklist before you commit to anything
- Be honest about what you actually want. Meaningful weight loss and a modest nudge are different goals requiring different tools; a microdose fits one of them, not both.
- Make sure a clinician, not a checkout page, is the one deciding the dose.
- Confirm a licensed pharmacy is dispensing it and will actually walk you through measuring it correctly.
- Get a way to track dose, weight, and side effects over time, otherwise you won’t know if it’s working or just feels like it is.
- Ask, seriously, whether a covered standard dose beats the microdose math on cost.
The honest bottom line
Microdosing a GLP-1 is a real tolerability accommodation and a weak strategy for maximizing weight loss. The data that exists shows a low dose beats placebo and loses badly to a full dose, and nothing has been directly tested on what a sustained low-dose protocol does over the long run. If your target is modest, or standard titration makes you sick, a supervised low dose is defensible, and FormBlends is where oversight and actual progress tracking are most built in, with HealthRX.com a close second. If your target is serious weight loss, the better bet is usually a properly studied dose done right, not a workaround engineered to feel gentler.
A few common questions
Will microdosing a GLP-1 actually get me meaningful weight loss?
Partially, and mostly not. The lowest dose ever formally studied, 0.05 mg of daily semaglutide, produced about 6% mean weight loss at one year, more than placebo, but less than half of what the higher studied doses achieved [1]. The 15% to 21% results that get all the attention came from full maintenance doses held for 68 to 72 weeks [2][3]. A deliberate microdose buys a fraction of the proven effect, not a discounted version of the same result.
Is GLP-1 microdosing FDA-approved?
No. There’s no FDA-approved microdosing indication, and no clinical trial has tested a deliberate microdose protocol for weight loss specifically. It’s off-label by definition, since it sits below the labeled starting dose. Claims about how well it works are extrapolated from dose-response data collected for other purposes, not measured in a microdosing trial, because none exists.
When does a low dose actually make sense?
When standard titration makes you too sick to continue. The nausea, vomiting, diarrhea, and constipation that drive dropouts cluster in the escalation phase, so holding at a lower dose to stay on the medication at all can outperform pushing higher and quitting. Clinicians already do a version of this and call it slow titration. It stops making sense the moment it becomes a permanent, cost-saving destination paired with an expectation of full-dose results.
How risky is measuring my own microdose?
Riskier than most people assume. Drawing a small self-measured amount from a multidose vial is precisely the setup behind the dosing-error reports on record: over 455 for compounded semaglutide, more than 320 for compounded tirzepatide as of early 2025, with some errors off by 5- to 20-fold [5][6]. That’s a safety issue first, and a consistency issue second, since a measurement mistake also undermines whatever plan you were following. A licensed pharmacy that actually counsels you on technique is doing meaningful work here.
Why does weight loss plateau on a microdose?
Because the effect builds over months, and only once the dose is high enough to meaningfully suppress appetite and slow gastric emptying. A microdose can produce an early modest loss and then stall, which gets misread as the drug failing. The trials hit their published numbers because participants climbed to and held a target dose for well over a year. A stall on a microdose usually means the dose was never high enough, not that something stopped working.
If cost is the reason I’m considering this, what should I look at first?
Whether a covered standard dose is actually available to you. If the appeal of microdosing is mostly financial, a prior-authorization team chasing insurance coverage for an approved brand like Wegovy or Zepbound may net a larger result for less money than assembling a lower-dose workaround.
What is GLP-1 microdosing, technically?
Taking a dose of a GLP-1 receptor agonist, like semaglutide or tirzepatide, that’s deliberately below the standard therapeutic range used in trials, in hopes of getting some appetite effect while avoiding some of the side effects. There’s no agreed-upon threshold for what counts as “micro,” which is part of why the practice is genuinely hard to evaluate cleanly.
Is GLP-1 just another name for Ozempic?
No. GLP-1 is a hormone your gut produces after eating; it signals the pancreas, brain, and stomach in ways that reduce appetite and regulate blood sugar. Ozempic is a specific brand-name drug, semaglutide, built to mimic that hormone. It’s one product in a class that also includes liraglutide, tirzepatide, and others. Calling every GLP-1 drug “Ozempic” is roughly like calling every tissue a Kleenex.
Can a microdose still suppress appetite at all?
Some, in some people. Standard prescribing protocols start low and titrate up for a reason, low doses aren’t inert. But the effect is generally dose-dependent, meaning less drug tends to mean a smaller effect. A minority of people report noticeable appetite changes at modest doses, but there’s no reliable way to predict beforehand whether you’ll be one of them without trying it under medical supervision.
Where do people actually source compounded GLP-1s, and is that legitimate?
Compounded semaglutide became widely available during the FDA shortage period, and quality varied enormously by source. The legitimate route runs through a licensed compounding pharmacy under physician oversight, with a provider reviewing your history before writing anything. Providers like FormBlends operate inside that accountable structure. What isn’t legitimate: research-chemical vendors or supplement sites selling peptides with no prescriber involved anywhere in the process, which carries real quality and safety risk.
References
- O’Neil PM, Birkenfeld AL, McGowan B, et al. Efficacy and safety of semaglutide compared with liraglutide and placebo for weight loss in patients with obesity: a randomised, double-blind, placebo and active controlled, dose-ranging, phase 2 trial. The Lancet, 2018;392(10148):637-649. Dose response across 0.05 mg to 0.4 mg daily; the lowest dose produced roughly 6% mean weight loss at one year versus about 2.3% on placebo, less than half the highest dose. PMID 30122305. https://pubmed.ncbi.nlm.nih.gov/30122305/
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1). New England Journal of Medicine, 2021;384(11):989-1002. Semaglutide 2.4 mg produced a 14.9% mean body-weight reduction at 68 weeks versus 2.4% on placebo. PMID 33567185. https://pubmed.ncbi.nlm.nih.gov/33567185/
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). New England Journal of Medicine, 2022;387(3):205-216. Mean reductions of 15.0% (5 mg), 19.5% (10 mg), and 20.9% (15 mg) at 72 weeks. PMID 35658024.
- Aronne LJ, Horn DB, le Roux CW, et al. Tirzepatide as Compared with Semaglutide for the Treatment of Obesity (SURMOUNT-5). New England Journal of Medicine, 2025. Tirzepatide produced a 20.2% reduction versus 13.7% for semaglutide at 72 weeks. PMID 40353578.
- Lambson JE, Flegal SC, Johnson AR. Administration errors of compounded semaglutide reported to a poison control center: Case series. Journal of the American Pharmacists Association, 2023;63(5):1643-1645. Patients self-administered up to ten-fold dosing errors from compounded vials. PMID 37392810.
- U.S. Food and Drug Administration. FDA alerts health care providers, compounders and patients of dosing errors associated with compounded injectable semaglutide products. FDA Drug Safety communication, 2024. Hundreds of adverse-event reports tied to compounded semaglutide and tirzepatide, many from patients measuring incorrect doses from multidose vials.
Written by Delia Nakamura, staff writer. Following the evidence to its honest limits. Last reviewed May 2026.
For informational purposes. Any new treatment should be reviewed by a licensed professional first.

 By
By